Reasons for surgery
Your surgeon can suggest to remove your thyroid gland for several reasons:
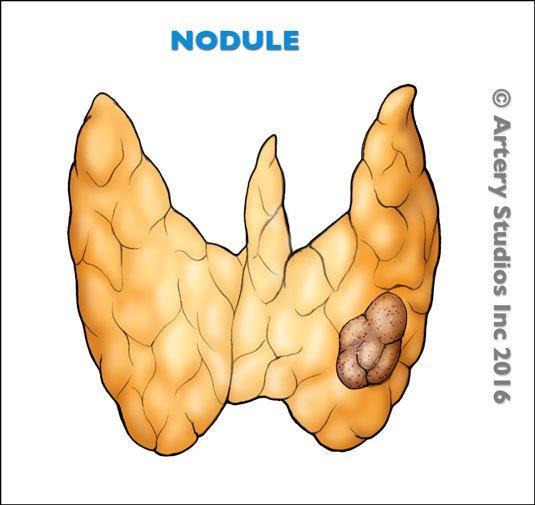
1. A suspected or proven thyroid cancer.
The majority of thyroid nodules are benign (non-cancerous) and should not cause any problems. If you have a thyroid nodule that is greater than 1 cm or has suspicious features on a neck ultrasound, your doctor or surgeon may recommend a fine needle aspiration biopsy (FNA) of the nodule.
The pathologists can give a probability of cancer depending on the cells they see when analyzing the biopsy tissue.
If they see only benign cells, your surgeon can decide to monitor the nodule with repeated ultrasounds and/or biopsies without the need for surgery.
If the cells are clearly malignant (cancerous), your surgeon may suggest removing part or all of the thyroid gland.
In a significant percentage of cases, the cells may be indeterminate and the pathologist cannot tell for sure if the nodule is benign or a cancerous. You will then have several options you will discuss with your surgeon:
- Active surveillance: If the probability of cancer is low or moderate, you and your surgeon can decide to follow the nodule closely with repeat ultrasounds and/or FNA and only chose to do surgery if it grows or shows signs of cancer.
- Genetic testing: There are now genetic tests available to give us more information about the tissue from the biopsy. Although they cannot guarantee if the cells are cancerous or not, they provide supplemental information to help you and your surgeon make a decision. You should know that these tests are not currently covered by OHIP (provincial healthcare insurance). Please talk to your surgeon if you want to learn more about genetic testing.
- Surgery:
- Remove only half of the gland first: Your surgeon may suggest removal of half of the thyroid gland containing the suspicious nodule and analyse it first. During the surgery, your surgeon will send some tissue for analysis (called frozen section analysis). If this tissue is cancerous, your surgeon may remove the other half of the gland during the same surgery. In most cases, the frozen section analysis at the time may not be able to tell for certain if cancer is present and you and your surgeon will have to wait for the final pathology results (usually available in 10-14 days). If cancer is identified on the final pathology report, your surgeon will discuss and recommend whether or not you will need a second operation to remove the remaining thyroid gland and possible adjacent lymph nodes if they are involved with cancer.
- Remove the whole gland: Your surgeon can also offer to remove the whole thyroid gland to avoid needing a 2nd surgery if it happens to be cancerous. Your surgeon will always discuss the pros and cons of this decision with you prior to the surgery and make sure to find a solution that best meets your needs and wishes.
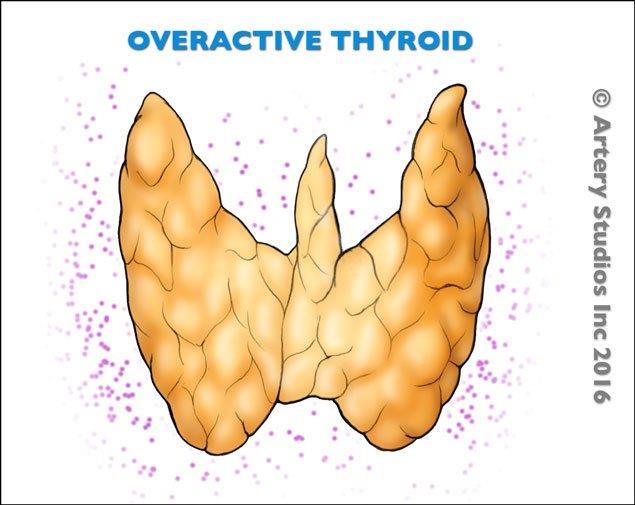
2. Hyperthyroidism not responding to medical treatment.
Hyperthyroidism of the entire gland (Grave's disease), or an overactive nodule are benign diseases that usually respond well to medical management (e.g. 'PTU', methamizole, radioactive iodine). If your disease is not responding well enough to the medications and your symptoms are debilitating, your surgeon can offer thyroid surgery to remove all or part of the thyroid gland depending on the disease.
3. A really large or growing thyroid gland (also known as a 'goitre') that puts pressure on surrounding structures
A goiter is a thyroid gland that is abnormally enlarged. Even if it is benign, it could cause serious symptoms if it is large enough to compress the adjacent structures such as:
- Your trachea (windpipe): Some patients can experience shortness of breath on exertion or even at rest if the goiter is very large
- The nerves to the larynx: Some patients can notice a hoarse voice due to the compression of the nearby nerves that control your voice box (recurrent laryngeal nerves).
- The oesophagus: Some patients can experience difficulty swallowing or the sensation of food getting stuck in the throat due to the goiter compressing the oesophagus (swallowing tube).
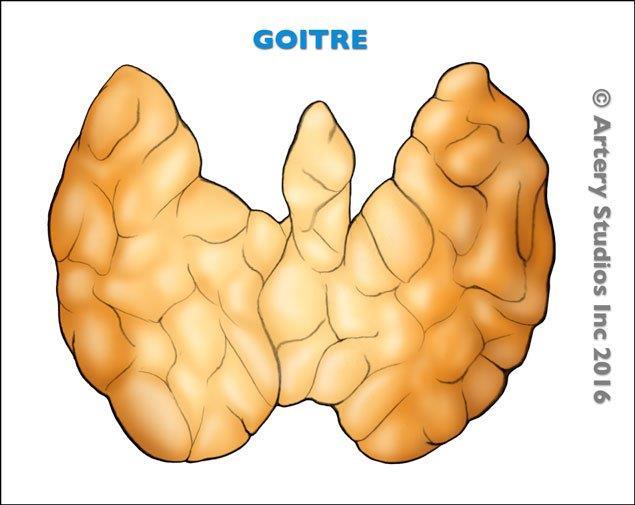
4. Goiter
If your goiter has slowly grown over the years and is causing significant aesthetic concerns, you can decide to have it removed, understanding the risks and implications of the surgery.
The majority of thyroid nodules are benign (non-cancerous) and should not cause any problems. If you have a thyroid nodule that is greater than 1 cm or has suspicious features on a neck ultrasound, your doctor or surgeon may recommend a fine needle aspiration biopsy (FNA) of the nodule.
The pathologists can give a probability of cancer depending on the cells they see when analyzing the biopsy tissue.
If they see only benign cells, your surgeon can decide to monitor the nodule with repeated ultrasounds and/or biopsies without the need for surgery.
If the cells are clearly malignant (cancerous), your surgeon may suggest removing part or all of the thyroid gland.
In a significant percentage of cases, the cells may be indeterminate and the pathologist cannot tell for sure if the nodule is benign or a cancerous. You will then have several options you will discuss with your surgeon:

